

By Shree Baphna, AsAmNews Staff Writer
INDIA-A second wave of the COVID-19 pandemic has been sweeping across India, unchecked, for nearly 3 weeks now. The situation is nothing short of a calamity. People are desperate and full of fear, and blame is being tossed from every direction, at every entity- some are cursing scientists, while others are blaming the government for its negligence.
Even the wealthy and well-connected are having immense trouble gaining admission into hospitals across the country. If this is the case for the upper class, imagine the state of those who are underprivileged or from marginalized communities. Inequality within India has always been an issue, but today we in the upper echelons of society have been brought back down with a humbling crash.
I have been incredibly lucky during this pandemic. I live in a highly cosmopolitan city called Bangalore, in southern India. I can afford a place to live, alone, with enough space for myself. I have a job that enables me to work from the comfort of my home, and I have access to technology and the internet to order my daily needs online, delivered right to my doorstep. I do not have to leave my house for anything. For many thousands of people in India who work daily-wage jobs or do not have access to as many resources, this is not the case.
Even though I live here, and I am experiencing this deadly wave unfold right in front of my eyes, I am still shielded by the privilege I hold. That being said, it does not take much to know that India’s situation is dire. It is important for those outside of it to have at least an idea of the danger and desperation faced by India’s citizens at this moment. To do this, and to better help myself understand what the nation is up against, I decided to interview a doctor on the frontlines.
LATEST STORIES





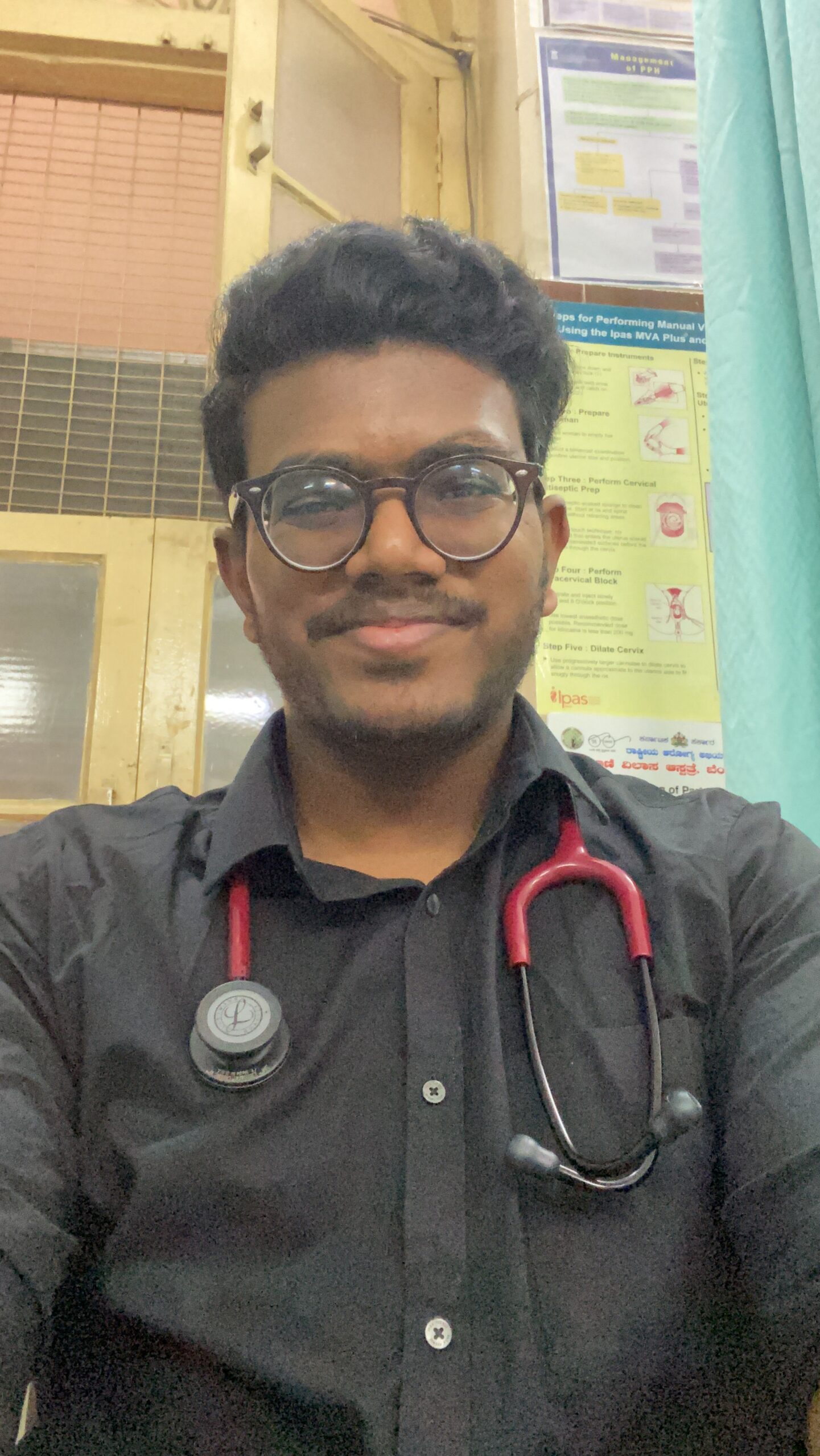
Dr. Harshith Dova is young. He is a recently graduated doctor working with a NGO. In India, medical school is a 5.5-year course you can undertake right out of high-school. Traditionally, 4th year medical students start doing clinical internships (after passing their final examination) in various departments on a rotational basis in order to get a better feel of the kind of medicine they would like to practice down the line. Given the current circumstances, many medical students have had their internship periods devoted solely to COVID-related healthcare.
I called Dr. Harshith (he prefers to be referred to as Harshith, which I will do so here on out) on an overcast Thursday afternoon. He had just returned from getting his second dose of the AstraZeneca vaccine- which in India is being developed under the name Covishield- when we began our conversation.
[Interviewer]: Harshith, do you get any days off if you feel a little under the weather because of the after-effects?
[Harshith]: No, I am still expected to show up for my shift, even if I am not feeling too well. In fact, I have a shift tonight that I hope I am not too tired for!
[Interviewer]: Goodness, that is not easy on you at all. I assume this is because hospitals are so severely short-staffed at the moment?
[Harshith]: Yes, that would be the case. This is in addition to the fact that vaccines too are in a shortage. As of now, there are a low number of Covaxin* doses available. The same goes for Covishield. Only those who need their second doses are allowed to obtain vaccine appointments.
[Interviewer]: Yes, especially for phase 3*, there will be a shortage of vaccines for a long time… the situation is really terrible.
[Interviewer]: What do you think are the biggest shortages the Indian healthcare system is dealing with?
[Harshith]: I would say the biggest thing is empathy. There is just a sheer lack of it within the healthcare system, and that is very important. Of course, there is also the extremely severe shortage of oxygen and vaccines. Almost all major hospitals run low on oxygen supplies on a daily basis.
However, I do think the government is mobilizing on this issue now, so there is an improvement in oxygen supply as compared to a few weeks ago. Hospital beds are also extremely tough to get. There are barriers at every stage in the process of gaining admission, which I will walk you through.

Now, usually what happens first, is that you take a COVID-19 test. Say you test positive; the next step is to obtain something called a BU number*. Next, using this BU number, a bed will be allotted to you in a hospital.
Sound pretty straightforward, right? It isn’t. There are so many hurdles at each stage. First of all, a hospital will only give a patient a bed if they have tested positive. For that, the patient must have access to testing facilities in the first place. Apart from that, an RT-PCR* test is only 80-85% accurate. This means that 15-20% of people may go undetected by the test. This margin of error causes patients to fall through the cracks. False negatives can stop someone from getting the treatment they need, because they need physical proof that they have been diagnosed with COVID-19*.
Next, say you have tested positive. It is time to get a BU number. However, given the usual state of bureaucracy and of course the sheer volume of people trying to get hospital beds, it will take a while to provide you with a BU number. This costs precious time within which a person’s condition can certainly deteriorate.
Then is the struggle of finding a hospital bed, which is extremely scarce. A patient may have to wait even longer after obtaining a BU number to find a hospital bed. This can further be detrimental to the patient’s state. If you are lucky and have found a hospital bed, however, there is no guarantee that a supply of oxygen will be available- which is what a growing number of patients really need right now. If things take a turn for the worse, and a patient needs an ICU bed, that is even more difficult to find. The worser a patient’s condition is, the harder it is to find the necessary treatment.
But that isn’t all. Even if the patient were able to obtain all the above treatment, they could still die. The cruelest irony is if the patient dies, their family members now have to cremate or bury the body, which entails waiting in line again. Crematoriums and burial grounds have reached their capacity. Families are either turned away or are forced to wait outside with a dead body in hand, for hours, until a cremation facility opens up. There is no dignity afforded to anyone, even in death.

[Interviewer]: The image you just painted…it’s just horrific. I’ve read in newspapers how the metal fixtures of crematorium facilities are actually melting because they have been burning with intense heat day and night.
[Harshith]: It is a nightmare indeed. And the worst part is, many of the patients falling severely ill are young.
[Interviewer]: This is definitely something we never really expected, did we? Given what you have just told me, how do these circumstances make you feel about your role as a doctor and frontline worker?
[Harshith]: Honestly, I have become quite disheartened with what I have seen or heard. Even worse, this role results in desensitization. When you see people dying at this rate, you might be on the verge of a mental breakdown, or you lose a sense of self. The worst part is, we have no choice but to push on and work like a robot. Or you just end up being very blunt about the situation.
The other thing that is most jarring- something which I have not had to do yet, thankfully- is to choose which patient gets to live. I have heard of this happening to other doctors at other hospitals, where two patients are waiting, but only one bed is available. For example, one patient is young and, in their twenties, whereas the other is patient is in their sixties and has a co-morbidity. On what basis can you make such a decision?
[Interviewer]: Wow…I can’t fathom having to make a decision like that. Let alone in 30 seconds.
[Harshith]: Yes. Going into this profession, I knew situations like this would arise at some point. But never at this speed, or at this scale.
[Interviewer]: Of course, this is literally a situation where you have a person’s life in your hands, and you have to decide this in a split second. It is near impossible…and then to have to explain as such to the patient’s family…
[Harshith]: Yes, it most certainly has repercussions for the patient’s family. We do not operate in isolation, which is what everyone must remember.
[Interviewer]: This leads me to a more personal question- how does your family feel, knowing that you are a frontline worker and are at risk of exposure every day?
[Harshith]: I think my family reacted the way most families would. My mother was not too happy about it. She is always discussing case numbers with me or informing me about how many positive cases were reported in the city on a particular day. My father is a little more reserved- he is worried of course but understands that this is my job and that I am doing what I have to do.
I think both of them- and this goes for me as well- do feel a sense of pride about the fact that I am a doctor working on the frontline. It is a privilege to be able to tackle a situation like this and to have the ability to help.
It is also important to note that I live apart from my family. As a result, I do not have the fear that many other doctors do of exposing their loved ones to this terrible virus. Knowing that I am not putting anyone at risk by doing my job gives me a little more confidence and determination in performing my duties.
[Interviewer]: I can certainly see why. I personally am in awe of frontline workers every day. The resilience and determination I see and hear of is heroic.
To change track a little, you mentioned a while back that frontline workers are at risk of mental or emotional breakdowns. What do you think frontline workers really need right now?
[Harshith]: They certainly need therapy, to be honest. Lots of mental and emotional support is necessary in the long-term. In a more short-term sense, we certainly need the government to start hiring more people or give the go-ahead to conduct the exams that will add more doctors to the existing pool.
Apart from more staff, we certainly need to acquire more vaccines on a larger scale and conduct vaccination more efficiently. Many people are actually oblivious to the fact that vaccines do work, and that even if one contracts COVID-19 after having been vaccinated, the case is usually very mild. Many patients that need hospitalization are those that have not been vaccinated. Therefore, picking up the pace on administering the shot would really help keep people safe from this infection.
[Interviewer]: I agree! I know some people are hesitant to take the vaccine because of all the commotion surrounding aftereffects. I guess the important thing to remember is that the very small chance of getting severe aftereffects is outweighs the other possibility of not getting vaccinated and then falling severely ill.
[Harshith]: Yes, exactly!
[Interviewer]: Given the shortage of tests and the number of people who are either not getting tested or are asymptomatic, how far off do you think reported case numbers are?
[Harshith]: You know to be honest; I had stopped looking at the numbers a long time ago, almost 6-7 months. It is quite disheartening to look at. It just increases the stress and pressure that frontline workers are under.
[Interviewer]: I completely understand. You know it is similar to how you mentioned frontline workers becoming desensitized to the situation. We non-medical people are very desensitized to the numbers in a certain way because it is very external to our lives. We just read it from a newspaper and go about the rest of our days. But for frontline workers, it is very different because you are immersed in patient-care day and night.
[Harshith]: Yes, exactly. But to answer your question, I cannot tell you a specific number, but I can tell you that there is a pretty good margin between actual case numbers and reported case numbers.
Do you mind telling me a little bit about yourself?
[Harshith]: I finished my internship period as a part of medical school in February this year. Currently, I work for a NGO while studying for something called post-graduate examinations. Passing this would allow me to become a resident. Right now, post-graduate medical students are being roped into COVID efforts. For undergraduate medical students, this means that even if they wanted to try and do our internship in another department- like surgery- everything is being diverted to fight the pandemic.
[Interviewer]: So, if the internship stage is meant for medical students to gain experience in the field they want to specialize in, are they now unable to get this exposure?
[Harshith]: Yes, the internship period cannot be re-done. Effectively, these medical students have forgone the opportunity of exposure and practical learning.
[Interviewer]: Is this all being done because of short-staffed healthcare facilities?
[Harshith]: Exactly. What is worse, is that to the government, post-graduate (PG) students are cheap labor. Instead of hiring expensive doctors, PG students are becoming scapegoats. Certified doctors are registered, compelling the government to pay them full-time. Post-graduate students, on the other hand, are expected to do the same work as these doctors and are paid nearly 20-30% less. On top of that, they are expected to pay full tuition for medical school they are not attending because of constant COVID-care duties.
[Interviewer]: That is terrible! I know in the United States, there is some scope of obtaining financial aid. Does something like that exist for medical students in India?
[Harshith]: Yes, kind of, but in the form of scholarships or grants. There is no governmental aid, per se.
[Interviewer]: Oh wow. It is hard, because students also have to take care of multiple other expenses, including school tuition.
[Harshith]: Yes. On top of that, a lot of undergraduate medical students have been performing telemedicine duties. This should ideally be performed by certified doctors. Even for this, medical students are paid extremely low salaries.
This problem could be solved to a certain extent. In order for medical students to become certified, registered doctors, they have to take the post-graduate exam, which in India is called the NEET-PG. If this exam were held, PG students could be added to the existing pool of full-fledged doctors, therefore reducing the strain of staffing shortages a little.
This is especially because most- if not all- teaching hospitals are run by resident doctors. In addition, it would stop this cruel exploitation of cheap labor, because as full-fledged doctors, they would be eligible for full pay from the government. But the government is refusing to hold this nation-wide exam because of the fear of spreading COVID.
Now, if the government can hold super-spreader events like election campaign rallies, or allow enormous religious gatherings, why won’t they hold this one exam that would allow some relief to the medical system? Effectively, the government is trying their best to postpone the exam for as long as possible so that they do not have to spend more money on more doctors.
[Interviewer]: The sheer hypocrisy of this horrendous. The government is trying to avoid giving medical students full working benefits just to cut corners, and they expect you to- quite literally- lay down your life for this country without question!
[Harshith]: Yes, pretty much. Here, the State-Level Association of Resident Doctors is trying to raise awareness of how much medical staff are being overworked. They have been posting videos explaining our plight. However, the only people watching these videos are the ones within the medical fraternity.
Our appeal has not caught the attention of those outside of this sphere. It’s funny, you know- the minute it comes to instigating change in a system that will surely require a lot more effort and impact people’s lives directly, no one wants to put in the work for it. But something like canceling the IPL (Indian Premiere League in cricket) garnered so much media coverage. Yet it is not something that affects our lives directly.
[Interviewer]: That is a very poignant comparison indeed. It is counterintuitive when we come to think of it, right? Something that is not even that important is given so much more attention than the state of our healthcare system.
[Interviewer]: Before we wrap up, is there anything else you would like to add or say?
[Harshith]: Just that people should get vaccinated and stay at home! There are so many people out there who refuse to do this, which puts others at risk. I find that older generations are more hesitant to take the vaccine than younger ones. Therefore, it falls on the younger generation to persuade their older family members to get vaccinated. It is very important that everyone does, and that everyone understands how the vaccine actually works. Besides that, please do help us raise awareness about the situation of medical students in India. We work tirelessly and deserve the same rights and benefits as all other medical professionals.
[END]
For more information about frontline workers and the kinds of work conditions they are facing, please watch (and share) these videos:
Acknowledgements: Thanks to Dr. Harshith Dova for taking the time amidst his busy schedule to do this interview with me. This article is one small way to raise awareness of what frontline workers in India and everywhere else are facing. Please read, share, and like this article. Our doctors, nurses, and community healthcare workers (who are majority women!) are risking their lives. Stay home, mask up, and get vaccinated- it is the least we can do.
Notes:
- Covaxin: This is the name of the indigenous vaccine developed in India by a company called Bharat Biotech
- Phase 3: India is conducting vaccination in phases, with phase 3 being those who are 18 years of age and above.
- BU number: Numbering system for patients who test positive in the city of Bangalore, India. BU stands for ‘Bengaluru Urban’, which is a district of Bangalore and refers specifically to those living in urban areas of the city.
- RT-PCR: Real time Reverse Transcription Polymerase Chain Reaction
AsAmNews has Asian America in its heart. We’re an all-volunteer effort of dedicated staff and interns. Check out our new Instagram account. Go to our Twitter feed and Facebook page for more content. Please consider interning, joining our staff, or submitting a story or making a contribution.
{kind=link}